Elbow Dysplasia

Four Hereditary Developmental Disorders
The term "elbow dysplasia" encompasses four different hereditary developmental disorders of the elbow joint, namely:
- The free anconeus process (LPA)
- The free medial coronoid process of the ulna (LPCM)
- Osteochondritis dissecans of the medial humeral condyle (OCD)
- Discrepancy between the articular surfaces of the radius and ulna and those of the humerus (INC)
These conditions can cause pain and lameness in large and medium-sized dog breeds. Only accurate diagnosis and prompt treatment can prevent the aforementioned conditions from leading to osteoarthritis and permanent lameness.
The anconeus process (LPA)
During normal development, the processus anconeus (PA) has a secondary ossification center that fuses with the ulna at 5–6 months of age. If the radius is relatively too long, the humerus may press against the PA, preventing it from fusing with the ulna.
This form of ED is often seen in young dogs starting at 6 months of age. The dogs show lameness in one or both front legs. Sometimes the elbow joint is effused and/or there is a pain response and crepitus upon hyperextension of the elbow.
Coronoid process (LPC)
The coronoid process (PC) is part of the radioulnar and humeroulnar joints. Joint incongruity and trauma can lead to detachment or fissures of the PC.
This hereditary condition is common in Labradors, Rottweilers, and Bernese Mountain Dogs. In 70% of cases, there is bilateral lameness; often, the joint is also effused, and there is tenderness and crepitus during passive movement of the elbow.
Osteochondrosis dissecans (OCD)
Osteochondrosis (OC) is caused by a disruption of enchondral ossification in the articular-epiphyseal complex. Nutrition plays an important role as an etiological factor. The condition is referred to as osteochondrosis dissecans (OCD) when loose pieces of cartilage or bone enter the joint.
The clinical signs closely resemble those of a LPC. However, in cases of OCD of the elbow, the dog often turns its paw outward to relieve pressure on the medial side of the joint. OC is commonly seen in young dogs of large breeds starting at 4–6 months of age.
Elbow Joint Incongruity
This may be caused by a relatively short ulna, causing the radius to press the humerus against the anconeal process and resulting in LPA. If the anconeal process is already bony and fused to the olecranon (at >6 months of age), the condition is known as distractio cuniti. This condition is very painful for the dog.
The radius may also be too short. In that case, the ulna will bear a greater load, which can lead to cartilage lesions and joint pain, resulting in osteoarthritis.
Diagnosis
- Breed and age can point toward a diagnosis (Note: Older dogs can also have ED and may not experience symptoms until later in life).
- Based on a thorough orthopedic clinical examination: unilateral or bilateral lameness, swelling of the elbow joint, tenderness, and crepitus during passive movements (hyperextension).
- X-rays of the elbow joints. LPA is often clearly visible on an X-ray. This is often not the case with LPC.
- If the X-ray shows no evidence of lameness, a CT scan of the elbow can provide clarity. Loose fragments are visible on a CT scan but usually not on an X-ray, especially if the fragments have not displaced, as is often seen in LPC.
CASE: Max, a Labrador Retriever, 8 months old, limping on his left front leg
This dog had been limping on his left front leg ever since he tripped over his leash. After resting for a while, the symptoms disappeared, but they returned over time. The pain was mainly felt when starting to move.
A clinical examination revealed that hyperextension of the left elbow was painful. The elbow was not swollen. Otherwise, the range of motion (ROM) was normal.
On the left below is an X-ray of the elbow. Nothing out of the ordinary. Max was sent home with an NSAID and instructions to rest. However, the dog continued to limp intermittently on his left front leg.
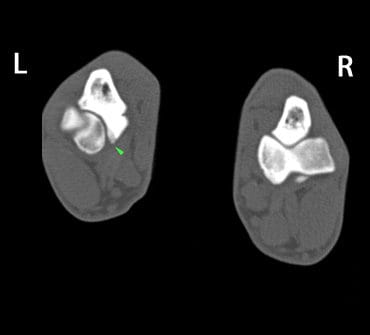
The attending veterinarian asked us to have a CT scan of Max’s elbows done. Based on the CT images (below right), he was diagnosed with LPCM on the left side.
Max was then referred to an orthopedic surgeon, and after surgery and a few weeks of rehabilitation, he was walking completely normally again.